Guides, leaflets and resources
Vulvodynia pre-clinic questionnaire
The vulvodynia pre-clinic questionnaire which follows can be printed out and completed by hand, or used as an aide-memoire in medical appointments. You can download a PDF version of the questionnaire using the links at the beginning and end of this page.
YOUR BACKGROUND
Name
Age
Date of birth
Number of children
Were these vaginal deliveries or caesarean sections?
If appropriate, did these deliveries affect your vulval symptoms?
❏ No Go to next question
❏ Yes Give details
Have you had any gynaecological problems in the past?
❏ No Go to next question
❏ Yes Give details
Any other health problems?
GENERAL LIFESTYLE
What is your present work or occupation?
Do you do any physical fitness activities?
❏ No Go to next question
❏ Yes Please list what, and how often
PRESENT VULVAL COMPLAINTS
What diagnosis do you have for your symptoms?
Please indicate the type of symptoms that you have (you can indicate one or more)
❏ Burning
❏ Soreness
❏ Irritation
❏ Itching
❏ Painful sex
❏ Vaginal discharge
❏ Other (please state)
Are your symptoms constant?
❏ Yes
❏ No
❏ Intermittent – good days and bad days
What bothers you the most about your problem?
How many months/years have you had symptoms?
How is your general energy level?
What do you clean the vulva with? How often do you wash/clean your vulva?
Have your doctors prescribed or recommended any medications?
❏ No Go to next question
❏ Yes Please give the names of all the substances that you can remember (including vaginal preparations, skin creams and pills)
Have you put anything not prescribed by a doctor on your skin yourself for treatment?
❏ No Go to next question
❏ Yes Please list
Can you remember what exactly caused your symptoms?
❏ No Go to next question
❏ Yes Please list
How are the symptoms you now have related to your initial symptoms?
❏ Same discomfort
❏ Less intense discomfort
❏ More intense discomfort
❏ Less frequent
❏ More frequent
Have you been free of symptoms at any time? For how long?
❏ No Go to next question
❏ Yes When?
Are there certain times of the day when your symptoms are more noticeable?
❏ Morning
❏ Evening
❏ Night (bedtime)
❏ Always throughout the day
❏ With urination
❏ After a bowel movement
Are there certain times of the month when your symptoms are more noticeable?
❏ Worse just before my menstrual period
❏ Worse during my menstrual period
❏ Worse just after my menstrual period
❏ Always the same during the month
❏ Worse when I ovulate (mid-cycle)
The discomfort which I most often have is
❏ Slight, I notice only when I think about it
❏ Slight, I can ignore it by not thinking about it
❏ Moderate, I always know it’s there but I can still perform most tasks
❏ Severe, it allows me to perform only tasks which require little concentration
❏ Severe, makes it impossible for me to do anything but seek medical attention
Please mark the squares which best show the location of your symptoms (a diagram and description of the different parts of the vulva are provided below for information)
❏ Mons pubis area
❏ Clitoris
❏ Labia majora
❏ Labia minora
❏ Urethra (bladder opening)
❏ Vestibule (inside the vulva)
❏ Vagina (within the vestibule)
❏ Perineum
❏ Anal area
Diagram showing the parts of the vulva
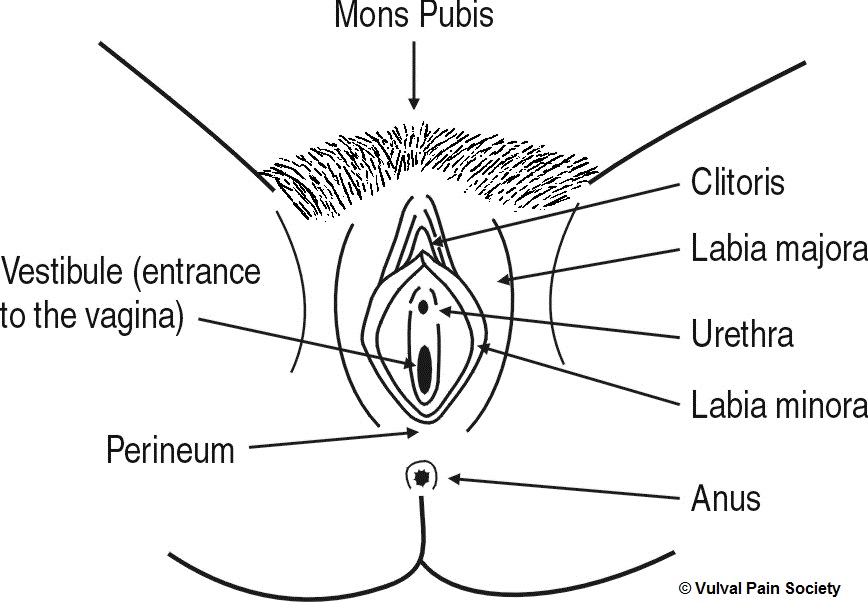
Explanation of the diagram
This is a black and white line diagram of the vulva. The vulva is viewed from the front, looking between the legs, with the woman lying on her back and the vulva spread open to show its inner parts.
Working from top to bottom of the diagram, so from the front to the back of the body, and from the outside inwards, the parts of the vulva shown are as follows:
- Mons pubis – the hairy, fatty triangular pad on the front of the body, just above the vulva
- Labia majora – the hairy, fatty outer lips containing the inner vulva
- Labia minora – the hairless, fatless inner lips inside and between the labia majora
- Clitoris – a pea-sized organ located at the top meeting point of the labia minora below the mons pubis
- Urethra – the opening used to pass urine, located between the labia minora, below the clitoris and above the vaginal opening
- Vestibule – the entrance to the vagina, located between the labia minora around the vaginal opening
- Perineum – the bridge of skin and muscle located at the bottom meeting point of the labia majora, between the vaginal opening and the anus
- Anus – the external opening to the bowel, located below and behind the perineum towards the back.
My discomfort usually causes
❏ NO interference with daily routine or planned activities
❏ SOME interference with daily routine or planned activities
❏ An interrruption in daily routine or planned activities
❏ Confinement to bed
❏ The pursuit of immediate medical attention
Are you currently in a relationship?
❏ Yes
❏ No
My symptoms
❏ Do not affect sexual intercourse for me
❏ Sometimes prevent me from sexual intercourse
❏ Completely prevent me from sexual intercourse
❏ Cause discomfort, but do not prevent sexual intercourse
❏ May or may not affect sexual intercourse, but I don’t know, as I am not sexually active
When/if my symptoms prevent sexual intercourse, we
❏ Avoid sexual intimacy altogether
❏ Are physically close, but avoid sexual contact
❏ Concentrate on my partner’s satisfaction
❏ Have relations as usual
❏ Other
Is your partner aware of your problems?
❏ No Go to next question
❏ Yes If yes, what is the reaction?
Have you ever ended a relationship due to your vulval symptoms?
❏ No
❏ Yes
Have you thought that your vulval symptoms might be related to
Injury? ❏ Yes ❏ No
Stress? ❏ Yes ❏ No
Thrush? ❏ Yes ❏ No
Cancer? ❏ Yes ❏ No
Infection? ❏ Yes ❏ No
Other possible causes?
Do you think that there are any factors in your diet that might aggravate your symptoms?
❏ No Go to next question
❏ Yes Please list
Have you had any problems with your back (current symptoms or past history)?
❏ No Go to next question
❏ Yes Please describe
Are you optimistic about the future?
❏ Yes, my pain will go at some stage
❏ Yes, I will learn to live with the pain
❏ No
Is there anything else you’d like to say about your vulval pain?
© Vulval Pain Society March 2016
We are grateful to the British Society for the Study of Vulval Disease (BSSVD) for their endorsement of this questionnaire.